It often begins with a moment that feels small but refuses to be ignored. One night, the erection fades too early. Another time, it does not come at all. You tell yourself it is stress, or tiredness, or age. Yet days later, everything seems normal again. Morning erections appear. Masturbation works. But with a partner, the same problem returns.
This back-and-forth confuses men of every age. Younger men panic because they feel “too young” for erectile dysfunction. Older men assume it must be physical and permanent. Many stop talking about it altogether. Instead, they search late at night, typing questions like how to tell if ED is mental or physical, hoping for clarity.
Erectile dysfunction is not one single condition. It is a symptom with different causes, timelines, and solutions. Some forms of ED begin suddenly, often after stress, anxiety, or a single bad experience. Others develop slowly, linked to blood flow, hormones, or long-term health issues. Many men fall somewhere in between, experiencing a mix of both.
Understanding the difference between psychogenic ED and physical ED is not about labels. It is about choosing the right path forward. When the cause is misunderstood, treatment often fails. When the cause is identified correctly, recovery becomes possible.
This guide breaks the confusion down into 7 clear signs, using real clinical logic, simple language, and evidence-based insights to help you understand what your body is actually telling you.
What Erectile Dysfunction Really Means
Erectile dysfunction is often misunderstood as a single problem with a single cause. In reality, ED is a symptom, not a disease. It reflects how well the brain, nerves, blood vessels, hormones, and emotions are working together at a given time.
Clinically, ED is divided into two broad categories: psychogenic and physical, also called organic ED. Psychogenic ED originates from psychological or emotional factors such as anxiety, stress, fear of failure, or relationship tension. Physical ED results from measurable biological issues like reduced blood flow, nerve damage, hormonal imbalance, or structural changes in penile tissue.
There is also a recognized clinical framework called psychogenic impotence classification, which helps doctors identify whether ED is primarily psychological, primarily organic, or mixed. Research shows that primary psychogenic ED occurs in approximately 3 in 9 men, especially in younger age groups, where physical disease is less common.
What many men do not realize is that mixed psychogenic organic ED is the most frequent real-world presentation. A mild physical change may trigger anxiety, and that anxiety then amplifies the problem. Understanding ED this way removes blame and replaces guesswork with clarity, which is essential for choosing the right treatment path.
Psychogenic ED vs Physical ED: At-a-Glance Comparison
One of the most effective ways to understand erectile dysfunction is to compare patterns, not isolated symptoms. Many men focus on a single experience, such as one failed erection or one successful morning erection, and draw the wrong conclusion. Clinicians instead look at consistency, timing, and context.
The table below highlights the difference between psychogenic ED and physical ED symptoms in a simplified, practical way.
Difference Between Psychogenic ED and Physical ED Symptoms Table
| Feature | Psychogenic ED | Physical (Organic) ED |
| Onset | Sudden, often following a stressful event or period of anxiety. | Gradual, developing slowly and subtly over months or years. |
| Progression | Fluctuates; it may work perfectly one day and fail the next. | Steady decline; it progressively worsens with time. |
| Morning Erections | Usually present and firm upon waking. | Often absent or significantly weaker than they used to be. |
| Nocturnal Erections | Normal during sleep (3–5 times per night). | Reduced or absent during sleep. |
| Masturbation | Usually normal; rigidity is high when alone. | Often impaired even during self-stimulation. |
| Role of Anxiety | Central factor; the primary cause of the dysfunction. | Secondary or entirely absent. |
| Medication Response | Strong initially, but may become inconsistent. | Partial or weak; requires higher doses or fails to help. |
This comparison shows why how to tell if ED is mental or physical depends on observing trends rather than single events. Psychogenic ED tends to be situational and variable, while organic ED shows steady decline. Many men fall between these two extremes, which is why mixed psychogenic organic ED is so common and often misdiagnosed.
The 7 Key Signs That Distinguish Psychogenic and Physical ED
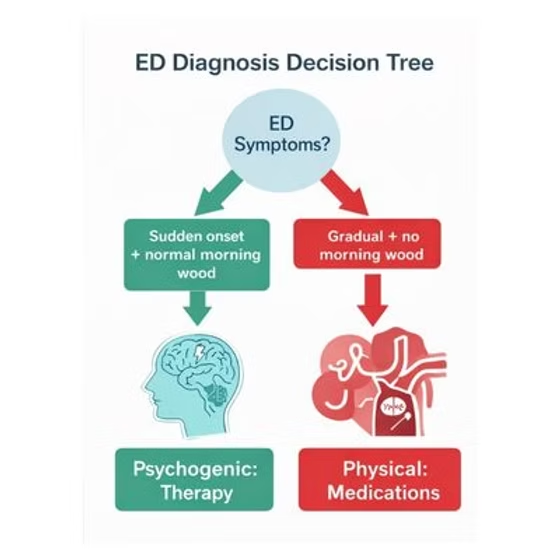
Key Sign 1: Onset Pattern — Sudden vs Gradual
One of the clearest ways to tell the difference between psychogenic ED and physical ED is how the problem began. The onset pattern often reveals more than any test.
Psychogenic ED usually has a sudden onset. Many men can point to a specific period or event when the problem started. This may include a stressful phase at work, a relationship conflict, a single episode of erection failure, or intense pressure to perform. Before this moment, erections were normal. After it, anxiety enters the picture. This pattern fits closely with psychogenic ED sudden onset vs gradual and is a key feature in psychogenic impotence classification.
In contrast, organic ED shows a gradual onset. Erections slowly lose firmness over time. More stimulation is needed. Morning erections become less frequent. Eventually, erections become difficult in all situations. This slow progression is typical of organic ED gradual onset and is commonly linked to blood flow problems, nerve damage, or hormonal changes.
Men with gradual decline rarely describe a single triggering event. Instead, they notice a steady change. Recognizing whether ED appeared suddenly or developed slowly is often the first and most important step in determining whether the cause is mental, physical, or mixed.
Key Sign 2: Morning Erections and What They Reveal
Morning erections, often called “morning wood,” are one of the most reliable natural indicators of erectile function. They occur during REM sleep and are not influenced by conscious thoughts, performance pressure, or anxiety. This makes them especially useful when trying to understand the cause of ED.
When morning wood is absent, particularly over many weeks or months, it often points toward physical ED. Reduced blood flow, nerve damage, or hormonal issues can prevent these spontaneous erections. This is why morning wood absent physical ED is considered a strong warning sign and often leads doctors to investigate vascular health, diabetes, or testosterone levels.
However, many men worry about whether anxiety alone can affect morning erections. So, can psychogenic ED cause no morning erections? The answer is yes, but usually temporarily. Severe stress, poor sleep, depression, alcohol use, or certain medications can suppress REM sleep, reducing morning erections even when physical structures are intact.
The key difference lies in duration. Temporary changes suggest psychogenic factors. Persistent absence strongly suggests a physical cause that should be medically evaluated.
Key Sign 3: Nocturnal Erections During Sleep
Most men are unaware that they experience erections while sleeping. During a normal night, men typically have three to five nocturnal erections during REM sleep. These erections occur automatically and are not influenced by conscious thoughts, anxiety, or sexual stimulation. This makes them one of the most important tools for understanding erectile dysfunction.
In cases of nocturnal erections psychogenic ED, these sleep-related erections remain normal. This indicates that blood flow, nerves, and erectile tissue are functioning properly. When a man has ED during waking sexual activity but normal erections during sleep, it strongly suggests a psychological or emotional cause.
Doctors often use the NPT test to distinguish psychogenic ED from physical ED. This test measures the frequency, firmness, and duration of nocturnal erections. Normal NPT results point toward psychogenic ED, while reduced or absent nocturnal erections suggest an organic cause.
Hormonal conditions also affect sleep erections. In men with low testosterone, or hypogonadism, NPT results may show weak or infrequent erections. This explains the link between hypogonadism and NPT tumescence and highlights why hormone testing is sometimes necessary.
Key Sign 4: Erections During Masturbation vs Intercourse
A very common and confusing experience for many men is having normal erections during masturbation but not during intercourse. This pattern is one of the strongest indicators that erectile dysfunction is psychogenic rather than physical.
Masturbation usually happens in a low-pressure environment. There is no fear of judgment, no expectation to perform, and no concern about satisfying a partner. The mind remains relaxed and focused on sensation. Because anxiety is minimal, the brain can send clear arousal signals, and erections occur normally.
During partnered sex, the situation changes. Thoughts such as “Will I stay hard?” or “What if I fail again?” can appear instantly. These thoughts trigger anxiety, which activates adrenaline and restricts blood flow. The erection weakens or disappears, even though physical ability is intact.
In some cases, excessive pornography use or masturbation addiction can contribute to psychogenic ED. Constant high stimulation may reduce arousal with real partners and increase performance pressure. This does not cause permanent damage, but it reinforces the psychological pattern behind ED.
Key Sign 5: Anxiety and the ED Performance Cycle
Anxiety plays a central role in many cases of erectile dysfunction, especially psychogenic ED. One of the most damaging patterns is known as the ED performance anxiety cycle, and once it starts, it can be difficult to break without the right approach.
The cycle usually begins with a single episode of erection difficulty. This may happen due to stress, fatigue, alcohol, or distraction. Instead of passing naturally, the experience creates fear. During the next sexual encounter, the man becomes hyper-aware of his erection. He starts monitoring firmness instead of feeling pleasure.
This mental focus triggers the body’s stress response. Adrenaline is released, which constricts blood vessels and directly interferes with erection. The erection weakens again, confirming the fear. Each repeated experience strengthens the cycle, making the problem feel permanent even when the body is physically capable.
This is why many men notice that pills help only temporarily. Medication may improve blood flow, but it does not stop anxious thoughts. Breaking the performance anxiety cycle requires reducing fear, restoring confidence, and retraining the brain to associate sex with safety rather than pressure.
Key Sign 6: Age, Health Profile, and Risk Factors
| Factor | Psychogenic ED (Mental) | Organic ED (Physical) |
| Typical Age Group | More common in younger men and early middle age. | More common after 40; risk increases with age. |
| Onset Pattern | Sudden, often linked to a specific stressor or anxiety. | Gradual, a slow decline over months or years. |
| Primary Triggers | Performance anxiety, fear of failure, chronic stress. | Diabetes, hypertension, vascular (heart) disease. |
| Lifestyle Influence | Porn overuse, relationship tension, mental fatigue. | Smoking, obesity, sedentary lifestyle. |
| Morning Erections | Usually present or inconsistent. | Often absent or progressively weaker. |
| Nocturnal Erections | Typically normal during REM sleep. | Reduced or absent during sleep. |
| Masturbation | Normal erections during masturbation but not intercourse. | Weak or absent even during masturbation. |
| Hormonal Role | Testosterone levels are usually normal. | Hypogonadism (Low-T) may be present. |
| Medical Testing | Limited, unless symptoms persist or causes are mixed. | Essential to assess blood flow and systemic health. |
Key Sign 7: How Your ED Responds to Treatment
How erectile dysfunction responds to treatment often reveals whether the cause is mental, physical, or mixed.
If ED Is Mainly Psychogenic
- Pills work well at first
- Erections improve on relaxed days
- Problems return during stress or pressure
- Results feel inconsistent
This happens because medication improves blood flow but does not remove anxiety. Studies show psychogenic ED responds to therapy CBT, which addresses fear and performance pressure directly.
If ED Is Mainly Physical
- Medication gives partial improvement
- Erections remain weak or unstable
- Higher doses are needed over time
- Effectiveness may decline gradually
If ED Is Mixed (Most Common)
- Pills support physical function
- Therapy stabilizes confidence
- Combined treatment works best
How your ED behaves over time often gives clearer answers than a single test.
Mixed Psychogenic–Organic ED: The Most Common Reality
Many men try to fit their erectile dysfunction into a single category, either mental or physical. In real life, this rarely works. The most common presentation doctors see is mixed psychogenic organic ED, where both factors are involved.
Mixed ED usually develops in stages:
- A mild physical change begins first, such as slightly reduced blood flow, early diabetes, or hormonal decline
- Erections become inconsistent rather than completely absent
- The man notices the change and begins to worry
- Anxiety increases during sexual activity
- Fear further reduces erection quality
Over time, the psychological component becomes stronger than the physical one. This is why some men say pills “sometimes work” but not always. The medication helps the physical side, but anxiety continues to interrupt arousal.
Mixed ED is often misdiagnosed because test results may look “borderline normal.” When anxiety is ignored, treatment stalls. The most effective approach addresses both components together, combining physical support with confidence rebuilding and anxiety reduction. When treated correctly, mixed ED is highly manageable and often reversible.
Relationship Stress, Porn Use, and Modern ED Triggers
Modern erectile dysfunction is not caused by health alone. Emotional connection, communication, and sexual habits now play a much bigger role than they did in the past.
Relationship stress is one of the most overlooked triggers of psychogenic ED. Unresolved arguments, emotional distance, fear of disappointing a partner, or lack of trust can quietly block sexual response. In such cases, psychogenic ED relationship issues treatment focuses on reducing pressure, improving communication, and restoring emotional safety rather than forcing performance.
Pornography use can also influence erectile function. Excessive or long-term exposure to high-stimulation content may reduce arousal with real partners. Over time, this can increase anxiety during intimacy and contribute to masturbation addiction psychogenic ED patterns. The issue is not masturbation itself, but dependence on unrealistic stimulation and constant novelty.
These modern triggers often coexist with stress, fatigue, and digital overload. Addressing them requires awareness and gradual change, not shame or extreme measures. When emotional and behavioral factors are corrected, sexual response often improves naturally.
How ED Is Treated Once the Cause Is Clear
Once erectile dysfunction is correctly classified as psychogenic, physical, or mixed, treatment becomes far more effective. The biggest mistake men make is starting treatment without understanding the underlying cause. Pills may temporarily mask symptoms, but they rarely resolve the core problem if the diagnosis is wrong.
Treatment Path for Psychogenic ED
When ED is psychological in origin, the primary issue is not blood flow but fear, conditioning, and anxiety patterns. In these cases, medication alone often creates dependency rather than recovery.
Evidence shows that psychogenic ED responds to therapy CBT in 75–85% of cases, especially when treatment focuses on:
- Breaking the ED performance anxiety cycle
- Reducing hyper-focus on erection quality
- Rebuilding confidence through gradual exposure
- Addressing relationship or intimacy-related stress
Structured psychosexual counselling helps retrain the brain to associate intimacy with safety instead of pressure. Temporary medication may be used as a support tool, but it is not the core solution.
Best Sex Therapist in India such as Dr. Dhruv Bhola focus on identifying anxiety-driven and mixed ED patterns early, helping patients avoid years of ineffective pill-based treatment by addressing psychological triggers, confidence erosion, and relationship dynamics through counselling-based care.
Frequently Asked Questions (FAQs)
Can psychogenic ED cause no morning erections?
Yes, psychogenic ED can temporarily cause reduced or absent morning erections, especially during periods of severe anxiety, depression, poor sleep, or high stress. These factors suppress REM sleep, where nocturnal erections normally occur. However, if morning wood is absent consistently for several months, physical causes such as vascular disease or hormonal imbalance should be evaluated.
How to tell if ED is mental or physical?
The easiest way to tell if ED is mental or physical is by looking at patterns. Sudden onset, normal erections during masturbation, and preserved nocturnal erections point toward psychogenic ED. Gradual worsening, morning wood absent, and difficulty in all situations suggest physical or organic ED. Doctors confirm this using history, labs, and tests like the NPT.
What does it mean if erections are normal during masturbation but not intercourse?
When erections are normal during masturbation but not intercourse, it strongly suggests psychogenic ED. Masturbation involves no performance pressure, fear of judgment, or emotional stress. During partnered sex, anxiety activates the fight-or-flight response, reducing blood flow and causing erection loss despite normal physical ability.
What is the difference between psychogenic ED and physical ED symptoms?
The key difference lies in consistency and onset. Psychogenic ED shows sudden onset, situational failure, normal nocturnal erections, and strong anxiety involvement. Physical ED shows gradual onset, consistent failure across situations, morning wood absent, and weak nocturnal erections. A structured symptoms table is often used to compare these patterns clearly.
Can masturbation addiction cause psychogenic ED?
Yes. Excessive masturbation combined with high-stimulus pornography can contribute to psychogenic ED. Over time, the brain becomes desensitized to normal intimacy, making real-life sexual situations less arousing. This is reversible through behavioral changes, reduced porn exposure, and therapy focused on dopamine reset and anxiety reduction.
What is the role of the NPT test in diagnosing ED?
The NPT (Nocturnal Penile Tumescence) test helps distinguish psychogenic ED from physical ED. Normal nocturnal erections suggest intact blood flow and nerve function, pointing toward a psychological cause. Abnormal or weak NPT results suggest organic ED, including vascular, neurological, or hormonal problems.
Does psychogenic ED respond to therapy CBT?
Yes. Research shows psychogenic ED responds to therapy CBT in about 75–85% of cases. Cognitive behavioral therapy helps break anxiety conditioning, reduce performance pressure, and rebuild sexual confidence. Medication alone rarely provides lasting recovery in these cases.
How common is psychogenic ED?
Primary psychogenic ED affects approximately 3 in 9 men, especially those under 40 years of age. It is strongly linked to performance anxiety, stress, relationship issues, and excessive porn exposure. This explains why most young men with ED do not have true organic disease.